In her free time, Nicole Lucas BSN, RN, CPUI, VA-BC™ volunteers at a local cat sanctuary. So far, she has adopted six.
This generous spirit bleeds into her career.
“I enjoy sharing my experiences with others: Helping new nurses become confident with IV insertion, providing tips and tricks I have learned throughout the years, seeing them succeed with a new skill,” Lucas said.
She has been working in her current vascular access team at Allegheny Health Network in Pittsburgh for 19 years.
“My favorite part of the job is the variety,” Lucas said. “Every insertion is different.”
She developed content for upcoming VACC’s Vein Preservation Program (VPP) which launches after the New Year.
“The VPP is important because vascular access is so much more than just sticking a patient,” Lucas said. “By obtaining the certificate, you are demonstrating your commitment to patient safety, satisfaction, and preparation for future needs.”
Her area of focus was Best Practices. This section discusses identifying a well-placed IV, understanding the impact medication has on veins, selecting the most appropriate catheter for a patient’s need, and much more.
When she received an email about volunteering for the program, she liked the idea of putting together an introductory guide of terms and rationale for any medical professional working with vascular access devices.
“Vascular access doesn’t always get the respect it deserves nor is the possible gravity of complications understood,” Lucas said.
Every day she encounters situations which inspire her content about Best Practices.
“Bedside nurses – particularly critical care and ER nurses always think bigger is better no matter what is being infused,” Lucas said. “I can’t count the number of times I’ve explained and demonstrated with pictures what is happening when there is a large catheter in a not so large vein.”
Three years ago, Ronald Fontano was precepted by Nicole.
“Everything I’ve learned about vascular access is because of her,” Fontano said. “Nicole taught me that inserting an IV is much more than a technical skill—it’s a thoughtful, patient-centered practice. She showed me that it’s about choosing the right vein, ensuring the safest option for the patient, and preserving vascular health to prevent future complications. Her guidance has profoundly shaped how I care for patients and think about vascular access.”
Betty Alcorn, MSN, RNH is the Nurse Manager at Allegheny Health Network. She says Nicole is always thinking outside the box. Once, a patient was ordered a PICC line for ordered TPN. The patient had a feeding tube at the time. The same day the PICC line was ordered, a consult for a speech was also ordered. Nicole contacted the Attending Physician and asked if the patient could wait a few days to see if she could maintain enough calories that the patient would not need a PICC line.
“This way the patient would not need an unnecessary procedure and incur the associated cost of the PICC placements,” Alcorn said. “Nicole aways looks out to the best interest of the patient.”
Volunteering for VACC is not the first time she has gone above and beyond. Ten years ago, she a was part of the team to spearhead the use of Midline catheters when appropriate instead of PICC lines – a pivotal moment in her career and another inspiration for the work with VPP.
The year was 2015. Her hospital began seeing an increase in acuity in the inpatient setting. The use of central lines – including PICC lines – increased in the hospital. With this increase in usage, the hospital saw an uptick in complications, including CLABSIs.
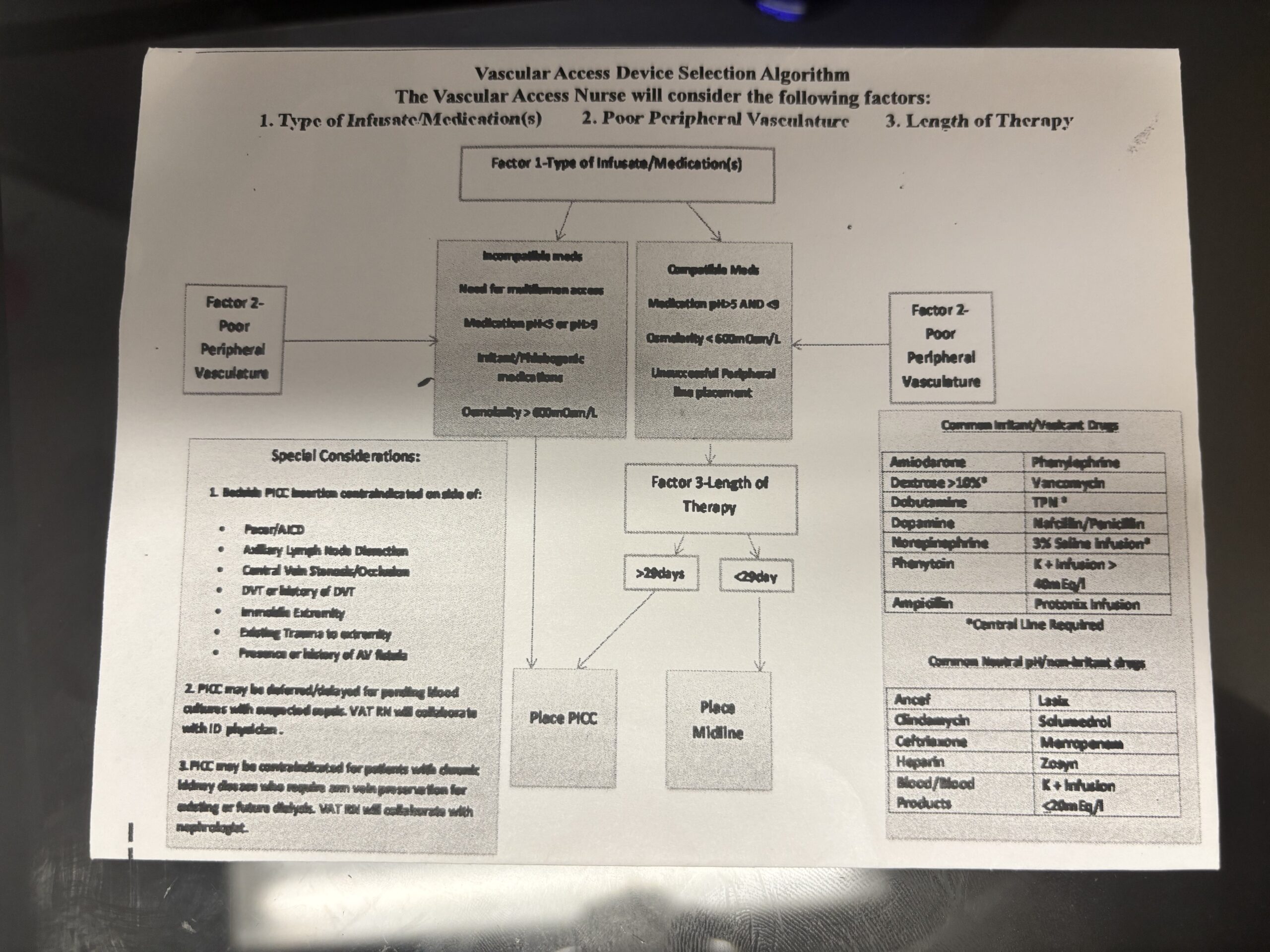
They created a simple graph asking questions about the patient’s plan of care including type of infusate, length of therapy, and the patient’s vasculature. Collaboratively, this allowed for the most appropriate line to be placed.
Prior to this protocol, there were no formal guidelines to determine the most appropriate line for a patient. If a physician ordered a PICC line, they were supposed to place it without discussion.
“Midlines were not often used because most physicians lacked the understanding of their use,” Lucas said.
She believes the biggest misconception when it comes to vascular access is its complexity.
“It is perceived by a lot of people as a simple task-oriented job,” Lucas said. “Feel vein, stick vein, task done. People don’t realize how much goes into placing the most appropriate line in a patient, from PT history to current plan of care, vessel size, vessel health, insertion angle, even to using the equipment! Not very simple!”
Once they created the algorithm, they had to present the flowchart to the medical executive committee (MEC) for approval.
“We did not receive a huge amount of pushback,” Lucas said. “The pushback we did receive was mostly related to a general knowledge deficit related to vascular access among physicians.”
Luckily, she had friends in high places. One of the Infectious Disease physicians they worked closely with was president of the MEC at the time. She welcomed the education they provided using MAGIC and INS standards.
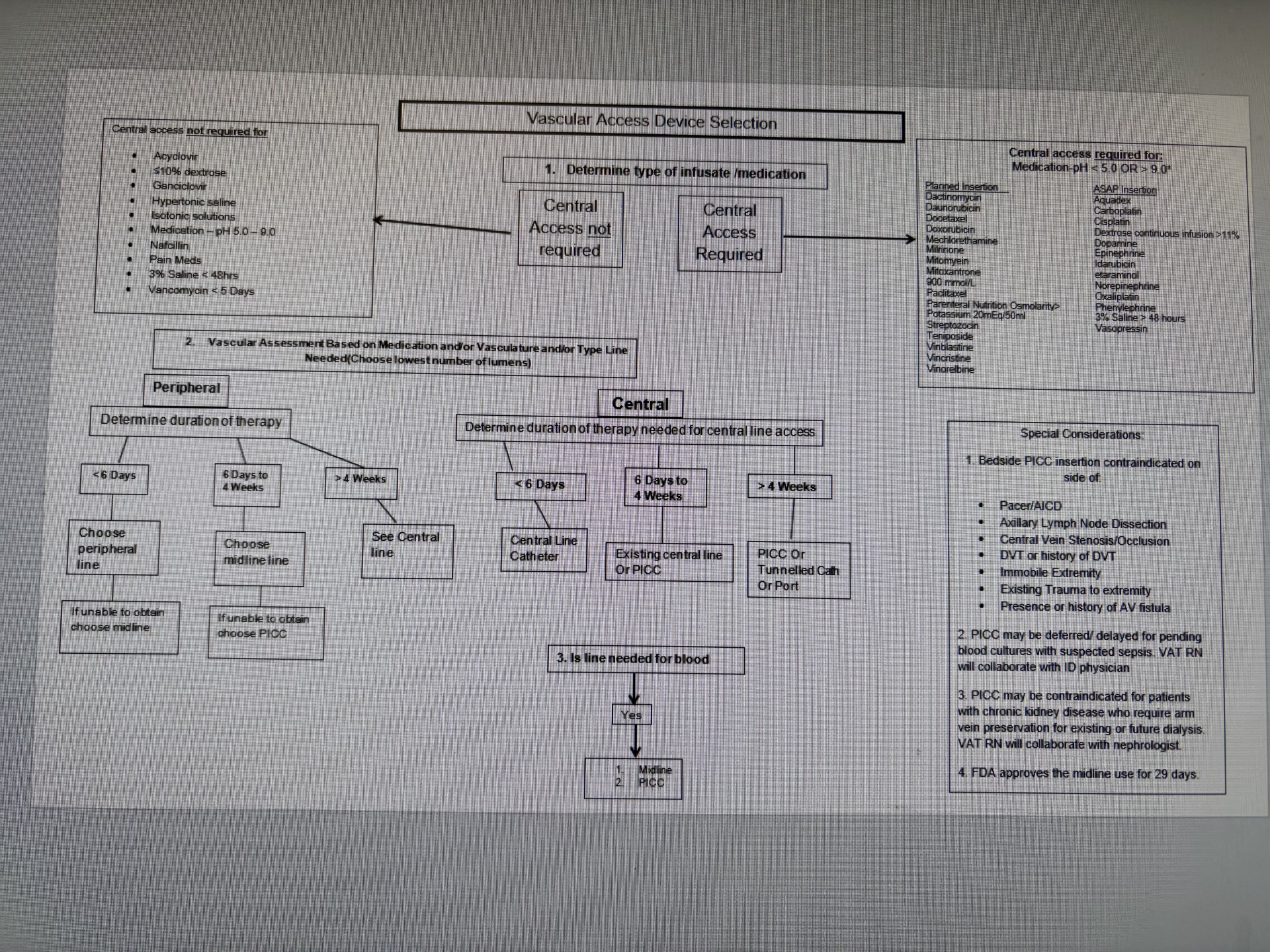 MEC approved the algorithm, and they implemented it in January of 2016. At the end of the calendar year, the hospital realized a 50% reduction in CLABSI and a 60% reduction in the number of central lines, including PICC lines inserted from the previous year. Central line days also dropped by almost 38%.
MEC approved the algorithm, and they implemented it in January of 2016. At the end of the calendar year, the hospital realized a 50% reduction in CLABSI and a 60% reduction in the number of central lines, including PICC lines inserted from the previous year. Central line days also dropped by almost 38%.
Through this process, she learned change can be difficult.
“It requires collaboration and patience,” Lucas said. “Sometimes the biggest barrier is education. Once we provided best practice guidelines with the rationale, it was easier for us to have an open conversation with physicians. We were able to utilize the algorithm to provide patient specific vascular access based on medical condition and patient needs.”
From there, the hard work was just beginning. She continues to write hospital policy and order procedure sets. Most recently, she got a nurse driven protocol to order upper extremity Dopplers approved.
“I like having direct input on my practice,” Lucas said.
In the past five years, they began implementing Ultrasound Guided IV insertion.
“We’re always learning as we go,” Lucas said. “We have a greater input in things than we used to.”
She got her VA-BC™ in June 2023.
“I had been putting it off,” Lucas said. “Did I know enough? Would the test be too hard?”
Her coworkers had been encouraging her to obtain it.
“I finally decided I should receive validation for all the work I was doing and needed it to pursue my clinical ladder,” Lucas said.
After nearly 30 years in the workforce, she still feels driven.
“I think what keeps me motivated is my desire to keep patients safe,” Lucas said. “I want to keep advocating for the right device at the right time and minimize complications.”
She has two pieces of advice for anyone starting out in vascular access. First, don’t become complacent.
“Keep reading the journals, watching webinars, and practicing your skills,” Lucas said. “Take the opportunity to go to conferences when possible.”
Second, be patient with yourself.
“You aren’t going to be successful with every patient, every time,” Lucas said. “Use those ‘failures’ to learn and adjust techniques, strengthen assessment skills.”